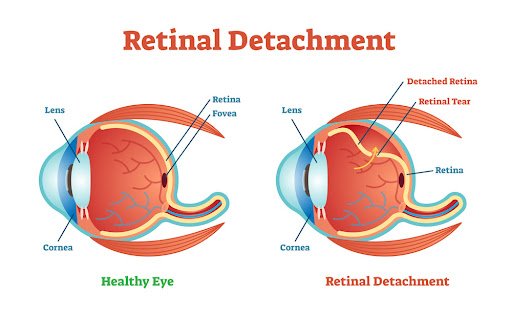
The retina, a thin layer of tissue at the back of the eye that processes light and sends visual signals to the brain, can detach from its normal position in a dangerous disorder known as retinal detachment. If left untreated, this detachment can impair the retina’s ability to function normally, resulting in a partial or whole loss of vision. Retinal detachment is regarded as a medical emergency even though it affects only 1 in 10,000 people annually.
Numerous reasons, like as ageing, eye traumas, or specific medical disorders like diabetes, can cause the condition. Early symptoms, like sudden light bursts, floaters, or a shadow covering your field of vision, must be identified in order to receive timely intervention.
Anatomy of the Retina
Gaining an understanding of the retina’s structure and function in vision is necessary before comprehending retinal detachment.
Retina
The retina is a layer of tissue that lines the inside surface of the eye and is sensitive to light. It takes in light that enters the eye and transforms it into electrical signals that travel via the optic nerve to the brain. We can see because of the brain’s processing of these impulses.
Photoreceptor Cells
Photoreceptor cells in the retina can be classified into two main types: rods and cones. Cones are in charge of colour and detail perception in bright light, while rods see in low light.
Macula
Sharp, detailed vision depends on the macula, which is located in the centre of the retina. For things like reading and recognising faces, it is necessary.
Retinal Layers
The retina is made up of several layers, one of which is the retinal pigment epithelium (RPE), which aids in maintaining the blood-retinal barrier and nourishes the photoreceptor cells. In addition, the RPE is involved in photopigment recycling and light absorption.
A probable loss of vision results from the retina’s detachment from the underlying tissue, which stops the retina’s blood supply. Seeking medical assistance right away is necessary to avoid long-term harm.
Types of Retinal Detachment
1. Rhegmatogenous Separation of the Retina
This variety makes up 90% of instances, making it the most prevalent. It happens when there is a rupture or hole in the retina, which permits fluid from the vitreous—the gel-like material that fills the eye—to seep beneath. The retina separates from the underlying tissue as a result of this fluid. Because the vitreous gel decreases and pulls away from the retina, rhegmatogenous detachment is frequently associated with ageing.
2. Retinal Detachment with Traction
This less common kind develops when the surface scar tissue of the retina contracts, causing the retina to move away from the rear of the eye. Proliferative diabetic retinopathy, a consequence of diabetes that causes aberrant blood vessel growth and the production of scar tissue, is most frequently linked to tractional separation.
3. Serous or Exudative Retinal Detachment
The accumulation of fluid behind the retina without a break or tear is known as exudative detachment. Tumours, vascular illnesses, or inflammatory conditions that result in fluid leaking can all produce this kind. There isn’t a palpable tugging on the retina like in the other forms.
Causes of Retinal Detachment
Many variables, frequently associated with the particular kind of detachment, can lead to retinal detachment:
- Ageing: As we become older, the vitreous gel in our eyes may thin and separate from the retina, resulting in holes or tears. The most frequent prelude to rhegmatogenous retinal detachment is this process, which is called posterior vitreous detachment (PVD).
- Eye Injuries: The retina may tear or separate as a result of trauma to the eye, such as a blow to the head. Additionally, injuries may cause internal eye haemorrhage, which raises the possibility of detachment.
- Previous Eye Surgery: Retinal detachment is more common in those who have had cataract surgery or other eye treatments in the past, particularly if there were issues during the procedure.
- Myopia: Also known as nearsightedness, individuals with extreme myopia have longer eyeballs, which can weaken and stretch the retina, increasing its vulnerability to rips and separations.
- Family History: An individual’s risk may be elevated by a family history of retinal detachment, suggesting a potential genetic susceptibility.
- Diabetic Retinopathy: In this condition, the retina develops aberrant blood vessels that have the potential to produce scar tissue. Tractional retinal detachment can result by pulling on the retina by this scar tissue.
- Inflammatory Disorders: A build-up of fluid behind the retina, such as uveitis (inflammation of the eye), can result in exudative detachment.
- Vascular Diseases and Tumours: Exudative detachment can be exacerbated by fluid leaks under the retina caused by systemic disorders such as hypertension or tumours within the eye.
Symptoms
- Light Flashes: Brief, abrupt light flashes in the periphery that are sometimes compared to lightning or sparks may be an indication of a retinal tear or separation.
- Floaters: A retinal tear or changes in the vitreous can be indicated by the emergence of new floaters, which are tiny, shadowy shapes that move across the field of vision.
- Shadow or Curtain Over Vision: One of the most common signs of retinal detachment is the movement of a black shadow or curtain across a portion of the visual field, which shows that the retina is pulling away from the underlying tissue.
- Blurred or Distorted Vision: If the macula, the core portion of the retina, is impacted, vision may become distorted, wavy, or blurry.
- Diminished Peripheral Vision: As the retina separates, side vision may be lost.
Diagnosis of Retinal Detachment
An expert in eye care must do a comprehensive examination in order to diagnose retinal detachment. To validate the diagnosis and ascertain the degree of separation, multiple examinations and instruments are employed:
Dilated Eye Exam
Using eye drops to dilate the pupil is the first step in diagnosing retinal detachment. This enables the ophthalmologist to use specialised lenses and lamps to examine the retina and vitreous more extensively.
Ophthalmoscopy
Tears, holes, or areas of detachment can be found in the retina with a thorough examination using an ophthalmoscope, a portable equipment having a light and magnifying lens.
Ultrasound Imaging
An ultrasound of the eye may be done if something, such as blood, is obstructing the view of the retina. This test helps determine the amount of the detachment by using sound waves to create an image of the inside of the eye.
Optical Coherence Tomography (OCT)
This non-invasive imaging procedure gives the doctor precise cross-sectional images of the retina, which they can use to evaluate the retina’s layers and thickness and identify any detachment or accumulation of fluid.
Treatment Options for Retinal Detachment
Surgery is usually necessary to treat retinal detachment; the precise procedure used will vary on the kind, location, and degree of the separation. Reattaching the retina and halting additional visual loss are the primary objectives.
Laser Photocoagulation
Laser surgery can be used to make tiny burns surrounding minor retinal tears or holes. Due to the scar tissue left over from these burns, fluid cannot pass through and detachment occurs because the retina is sealed off from the underlying tissue.
Cryopexy
In this treatment, a cryoprobe is used to freeze the region surrounding the retinal tear. Scar tissue formed by the freezing aids in the retina’s reattachment to the back of the eye. Cryopexy is frequently used with other surgical techniques.
Pneumatic Retinopexy
In Pneumatic Retinopexy, the vitreous cavity of the eye is pumped with a gas bubble. The detached retina is pressed up against the eye wall by the floating bubble. After that, the retina is fixed in place using a laser or cryotherapy. To keep the bubble in contact with the detachment, the patient needs to keep their head in a particular position for a few days.
Scleral Buckling
This surgical method entails encircling the outside of the eye with a silicone band, or buckle. By indenting the eye wall, the buckle releases tension on the retina and facilitates its reattachment. Scleral buckling is frequently used in conjunction with cryotherapy or laser therapy.
Vitrectomy
Surgery may be required in more complicated instances, such as those with massive detachments or tractional retinal detachments. In order to press the retina back into position, the vitreous gel is withdrawn from the eye and replaced with silicone oil or a gas bubble during this treatment. Over time, the gas bubble in the eye gradually fills with fluid; alternatively, a subsequent surgical procedure may be required to remove the silicone oil.
The risks and benefits of each treatment option vary, and the circumstances of the separation will determine which technique is best. To preserve as much vision as possible, prompt surgical intervention is essential.
Prevention Strategies
- Frequent Eye Exams: Regular eye exams can help identify early indicators of retinal abnormalities before they proceed to detachment, especially for people with excessive myopia, a family history of retinal detachment, or other risk factors.
- Protective Eyewear: Retinal detachment can be avoided by wearing protective eyewear when participating in sports or other activities that could cause eye injuries.
- Control of Chronic Conditions: Since diabetes and hypertension can aggravate conditions like diabetic retinopathy, which raises the risk of tractional retinal detachment, it is imperative to manage these conditions.
- Awareness of Symptoms: Understanding the early signs of retinal detachment, such as light flashes, floaters, or a shadow over the field of vision, can help in getting care quickly, which can reduce the chance of vision loss.
Potential Complications
- Loss of Vision: If retinal detachment is not promptly and successfully treated, the loss of vision might become permanent and irreversible.
- Recurrent Detachment: The retina may sometimes re-detach after surgery, necessitating further operations.
- Scar Tissue Formation: Following surgery, scar tissue may form on the surface of the retina, resulting in a condition called proliferative vitreoretinopathy (PVR), which can impair vision and necessitate further treatment.
- Infection or Hemorrhage: There is a minor risk of infection or haemorrhage, just as with any operation.
- Cataract Development: Cataracts are a frequent side effect of procedures like vitrectomy, particularly when gas or oil is used during surgery.
Prognosis and Follow-Up
Retinal detachment has a prognosis that varies according to the severity, how long it has been untreated, and whether the macula, which controls central vision, is involved. The likelihood of regaining vision increases with earlier intervention. However, even with treatment, some patients could have some vision loss. Follow-up care is essential for monitoring the healing process, resolving any difficulties, and ensuring the retina is still attached.
Conclusion
Retinal detachment is a serious eye disorder that can cause permanent vision loss. Understanding the anatomy of the retina, recognising the early signs of detachment, and obtaining quick medical attention are essential for preserving vision. Surgery is the main treatment, and several methods are employed based on the type and severity of the detachment. Retinal detachment can be prevented by maintaining regular eye exams and being aware of risk factors, but if it does develop, quick surgery can considerably enhance the prognosis.