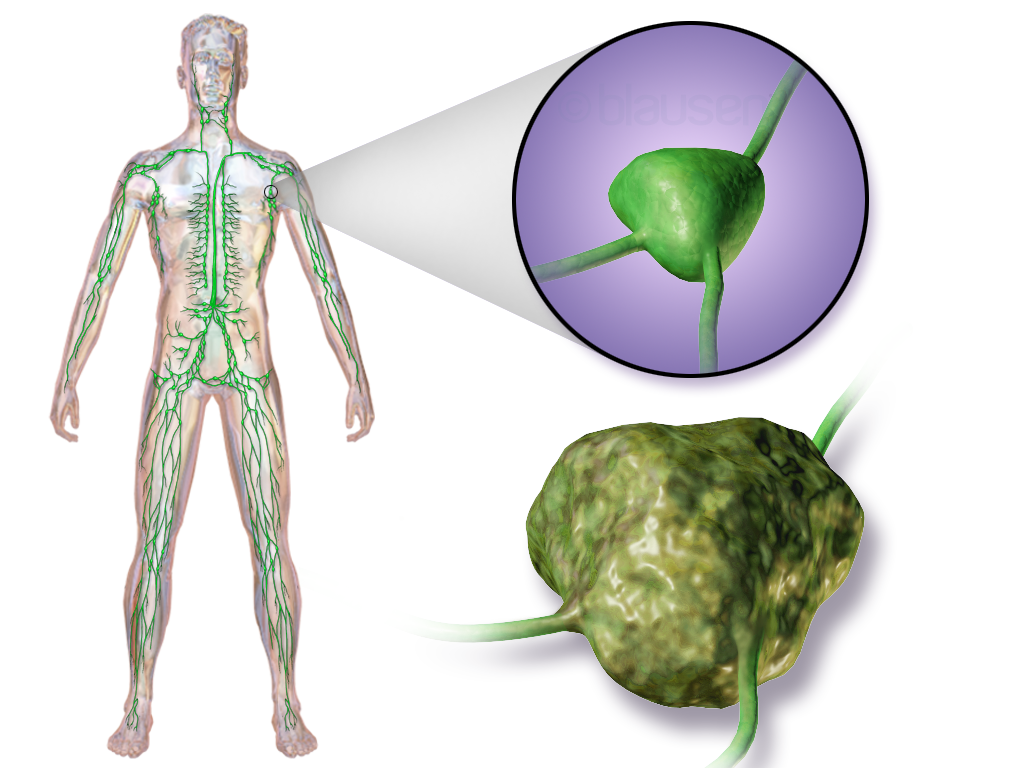
One kind of cancer that starts in the body’s lymphatic system—a system that is a component of the immune system—is lymphoma. White blood cells called lymphocytes are the main target of it. The spleen, bone marrow, lymph nodes, and other organs can all be impacted by lymphoma. Hodgkin lymphoma and non-Hodgkin lymphoma (NHL) are the two primary forms of lymphoma.
Types of Lymphoma
1. Hodgkin Lymphoma (HL)
- Features: Distinguished by the existence of Reed-Sternberg cells.
- Subtypes: Consists of nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) and classical Hodgkin lymphoma (CHL).
- Epidemiology: More prevalent in older individuals and young adults. Somewhat more prevalent in men.
- Symptoms: Frequent manifestations include fever, nocturnal sweats, weight loss, and painless lymph node swelling.
- Treatment: Usually includes radiation therapy, chemotherapy, and occasionally stem cell transplants.
2. Non-Hodgkin Lymphoma (NHL)
- Features: Consists of an assortment of lymphoid cancers.
- Subtypes: Separated into T-cell lymphomas (such as peripheral T-cell lymphoma, anaplastic large cell lymphoma) and B-cell lymphomas (such as diffuse large B-cell lymphoma, follicular lymphoma).
- Epidemiology: More prevalent and age-neutral than Hodgkin lymphoma.
- Symptoms: There is a wide range of symptoms that may include fever, weight loss, stomach pain, and swollen lymph nodes.
- Treatment: Treatment options for NHL vary depending on its particular type and stage. These may include immunotherapy, chemotherapy, targeted therapy, and occasionally stem cell transplantation.
Diagnosis
- Physical Examination: Assessment of various symptoms, including enlarged lymph nodes.
- Imaging Tests: MRI, PET, or CT scans to determine the severity of the illness.
- Biopsy: Tissue samples from afflicted lymph nodes or other regions are inspected under a microscope to confirm the existence of lymphoma cells.
- Blood Tests: These could include assays for certain lymphoma markers, lactate dehydrogenase (LDH) levels, and complete blood counts (CBC).
- Bone Marrow Biopsy: This is done to determine whether lymphoma has reached the bone marrow.
Staging
The process of staging lymphoma aids in assessing the disease’s severity and directs therapeutic choices. The stages consist of:
- Stage I: One organ or one lymph node region is affected.
- Stage II: Two or more lymph node areas on the same diaphragmatic side are involved.
- Stage III: Both sides of the diaphragm’s lymph node areas are affected.
- Stage IV: Widespread involvement of one or more organs that are not lymphatic (liver, bone marrow, etc.).
Treatment
1. Chemotherapy
- Description: Uses anti-cancer medications to eradicate cancer cells or inhibit their growth.
- Administration: Given intravenously or orally.
- Typical Regimens: ABVD (Adriamycin, Bleomycin, Vinblastine, Dacarbazine) associated with Hodgkin lymphoma. Non-Hodgkin Lymphoma: Rituximab (R-CHOP) is frequently used in conjunction with CHOP (Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone).
- Adverse Reactions: Weariness, nausea, vomiting, baldness, higher risk of infection, and possible long-term consequences such as cancer recurrence and infertility.
2. Radiation Treatment
- Synopsis: Using high-energy radiation to kill cancer cells. Usually in conjunction with chemotherapy for early-stage Hodgkin lymphoma.
- Method: Most frequently, external beam radiation is employed, directed towards the afflicted lymph nodes and their environs.
- Adverse Reactions: Skin irritation, exhaustion, nausea, possible harm to surrounding organs, and a higher chance of developing secondary malignancies.
3. Targeted Therapy
- Description: Medications made to specifically target chemicals needed for the development and viability of cancer cells.
- Examples: Rituximab (targets B-cell lymphomas’ CD20 protein), Ibrutinib (used in some B-cell lymphomas), Brentuximab vedotin (targets CD30 in relapsed or resistant Hodgkin lymphoma).
- Adverse Reactions: Varies based on the medicine in question, but may include blood cell count irregularities, allergic reactions, and infections.
4. Immunotherapy
- Categories:
- Checkpoint Inhibitors: Drugs like nivolumab and pembrolizumab block immune response-inhibiting proteins.
- CAR-T Cell Therapy: For example, axicabtagene ciloleucel is used in large B-cell lymphoma by modifying the patient’s T cells to target lymphoma cells.
- Adverse Reactions: Immune-related side effects, such as inflammation, cytokine release syndrome, and neurotoxicity.
5. Stem Cell Transplantation (SCT)
- Overview: Replaces unhealthy bone marrow with healthy stem cells.
- Categories:
- Autologous SCT: Utilizes the patient’s own stem cells.
- Allogeneic SCT: Uses donor stem cells.
- Method: Involves harvesting stem cells, administering a high-dose therapy to eradicate cancer cells, and injecting healthy stem cells.
- Adverse Reactions: Risk of infection, long-term consequences, and graft-versus-host disease (for allogeneic transplantation).
6. Alternative Treatments
- Natural Antibodies: Treatments like polatuzumab vedotin and obinutuzumab target specific antigens on lymphoma cells.
- Immunoradiotherapy: Combines immunotherapy (such as ibritumomab tiuxetan) with radiation therapy.
- Steroids: Used alongside other therapies to reduce immune response and inflammation.
Treatment by Stage
Early-Stage Hodgkin Lymphoma (Stage I–II)
- Often treated with a combination of chemotherapy and radiation.
- ABVD chemotherapy regimen followed by localized radiotherapy.
Advanced-Stage Hodgkin Lymphoma (Stages III–IV)
- More intensive chemotherapy regimens (e.g., escalated BEACOPP).
- Possible radiation for bulky disease.
Indolent Non-Hodgkin Lymphoma
- Often monitored until symptoms arise (watchful waiting).
- Chemotherapy alone or in combination with rituximab (R-CVP: rituximab, vincristine, cyclophosphamide, and prednisone).
Aggressive Non-Hodgkin Lymphoma
- Intensive chemotherapy regimens (e.g., R-CHOP).
- Consideration of stem cell transplantation for relapsed or refractory disease.
Prognosis
The prognosis for lymphoma varies greatly depending on the type of lymphoma, the patient’s age, general health, and response to treatment. While many non-Hodgkin lymphoma types have a worse prognosis than Hodgkin lymphoma, both types benefit greatly from early identification and treatment.
Follow-Up Care
Long-term follow-up care is usually necessary for lymphoma patients in order to monitor for recurrence or side effects after treatment. This could involve routine physical examinations, imaging scans, and lab work.
Conclusion
Lymphoma is a cancer that starts in the lymphatic system, affects lymphocytes, and spreads to different parts of the body. It mainly consists of non-Hodgkin lymphoma (NHL) and Hodgkin lymphoma (HL), each having unique characteristics and therapeutic modalities. Chemotherapy and radiation therapy are frequently used to treat Hodgkin lymphoma, but the course of treatment for NHL depends on the kind and stage of the disease and may include immunotherapy, chemotherapy, targeted therapy, and stem cell transplants. To improve results, precise diagnosis, tailored treatment regimens, and staging are essential. Although the prognosis varies, survival rates are greatly increased by early discovery and treatment. Long-term follow-up is necessary to manage treatment-related side effects and possible recurrences.