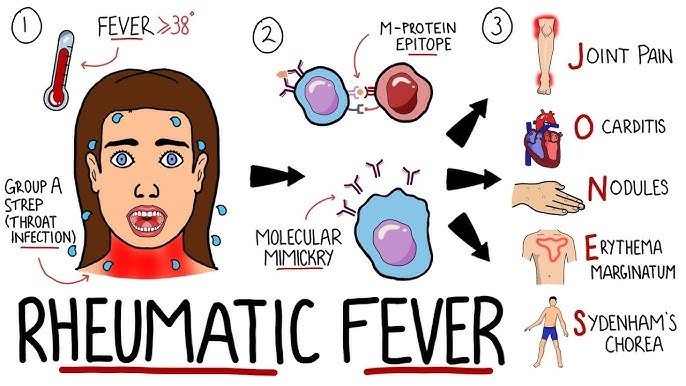
The inflammatory illness known as rheumatic fever (RF) can arise as a side effect of a streptococcal throat infection that is either untreated or not sufficiently treated (caused by Group A Streptococcus bacteria). Although it can strike adults, children between the ages of 5 and 15 are the primary victims of this illness. A major contributing factor to acquired heart disease in adolescents and young people worldwide, particularly in developing nations, is rheumatic fever.
Pathophysiology
Rheumatic fever is an autoimmune disease caused by the immune system’s reaction to a streptococcal throat infection. The immune system unintentionally attacks the body’s own tissues, including the heart, joints, skin, and central nervous system, instead of just the germs. Although the precise process is unknown, it is thought to be mostly dependent on molecular mimicry, where the immune system misinterprets bacterial antigens in the body’s own tissues.
Causes of Rheumatic Fever
1. Streptococcal Throat Infection (Group A Streptococcus)
- Primary Trigger: Untreated or insufficiently treated streptococcal throat infection is usually the cause of rheumatic fever. The immune system of the body launches an attack against the germs, but occasionally, in the process, it accidentally targets the body’s own tissues—most notably, the brain, joints, skin, and heart.
- Molecular Mimicry: Some of the streptococcal bacteria’s antigens, such as the M protein, resemble proteins that are present in human cells. Because of these similarities, the immune system becomes confused and attacks the germs as well as the body’s own tissues, causing inflammation and damage.
2. Delayed or Inadequate Treatment
- Inadequate Antibiotic Therapy: The bacteria may survive and continue to cause an immunological response if the original streptococcal infection is not completely treated with the recommended course of antibiotics. Rheumatic fever risk increases with incomplete or delayed therapy.
- Lack of Medical Access: Streptococcal infections frequently go untreated in many parts of the world, particularly in low- and middle-income nations, and this raises the incidence of rheumatic fever.
3. Genetic Predisposition
- Genetic Susceptibility: Rheumatic fever does not always follow a streptococcal throat infection. Some people are more prone to get the sickness because they are genetically inclined to have an overreaction to the infection in their immune systems.
- Family History: The chance of acquiring rheumatic fever or rheumatic heart disease is increased in families with a history of the disorder, indicating the possible involvement of specific hereditary elements.
4. Environmental Factors
- Overcrowding: Streptococcal infections are more likely to spread when living in close quarters. Dormitories, schools, and other close-knit settings are frequently the areas where strep disease can spread quickly.
- Poor Sanitation and Hygiene: Communities with limited access to clean water and sanitation systems are especially vulnerable to the spread of streptococcal germs due to inadequate hygiene practices.
5. Recurrent Streptococcal Infections
- Recurrent Episodes: People with a history of strep throat are more likely to develop rheumatic fever. Every infection that goes untreated or is treated insufficiently raises the risk of starting the autoimmune reaction that results in the disease.
Symptoms
Jones Criteria:
- Carditis: Indications of inflamed heart, such as shortness of breath, chest pain, or a recent heart murmur.
- Polyarthritis: Arthritis that migrates and affects several big joints at once.
- Sydenham Chorea: Characterized by abrupt, erratic, and uncontrollable movements, primarily affecting the hands, feet, and face.
- Erythema Marginatum: A rash that resembles a ring but is not irritating.
- Subcutaneous Nodules: Painless lumps beneath the skin, typically over the spine or joints.
Minor Criteria:
- Fever Arthritis: Pain in the joints without edema.
- Increased Acute Phase Reactants: Such as CRP and ESR.
- Prolonged ECG PR Interval: Diagnostic criteria include two main criteria or one major and two minor criteria, along with proof of a prior streptococcal infection.
Diagnosis
- Rapid Antigen Test or Throat Culture: To verify the existence of Group A Streptococcus.
- Antistreptolysin O (ASO) Titer: An elevated level suggests a recent infection with streptococcal bacteria.
- Echocardiography: To evaluate the involvement of the heart, especially valvular injury.
- ECG: To identify irregularities in cardiac rhythm.
Treatment of Rheumatic Fever
1. Antibiotic Therapy
- Elimination of Streptococcal Illness: The primary goal is to eliminate Group A Streptococcus bacteria. The preferred antibiotic is penicillin.
- Penicillin: Available as benzathine penicillin intramuscular injection as a single dose or as oral penicillin V for ten days.
- Options: Other antibiotics such as erythromycin, azithromycin, or clindamycin can be administered to people allergic to penicillin.
- Stopping the Recurrence: Prophylactic use of antibiotics over an extended period is required to prevent recurrent rheumatic fever episodes and further heart damage.
- Prophylaxis: The usual method is to inject benzathine penicillin intramuscularly every three to four weeks. The duration of prophylaxis depends on the severity of the initial episode and the presence of rheumatic heart disease (RHD).
- Prophylaxis Duration: Without cardiac symptoms, prophylaxis is continued for five years or until age twenty-one, whichever comes first. In cases with carditis but no residual heart disease, it continues for ten years or until age twenty-one. For residual heart disease, prophylaxis may last up to ten years or even for a lifetime.
2. Anti-inflammatory Medications
- Aspirin: High-dose aspirin is frequently used to reduce inflammation and ease pain in polyarthritis.
- Dosage: Adjusted based on the severity of symptoms, treatment continues until symptoms subside.
- Adverse Effects: Potential adverse effects, such as bleeding or gastrointestinal distress, must be closely monitored.
- Corticosteroids: Used when aspirin is insufficient to reduce inflammation or in severe cases of carditis.
- Prednisone: A corticosteroid commonly used to lower immune system activity and inflammation.
- Tapering: Corticosteroids are tapered off gradually when symptoms improve.
3. Supportive Care
- Bed Rest: Advised during the acute stage, especially for patients with carditis, to promote healing and reduce heart strain.
- Fluid Control: Careful management may be needed in severe carditis cases associated with heart failure to prevent overworking the heart.
4. Management of Complications
- Rheumatic Heart Disease (RHD): Patients with significant heart valve damage may require additional care.
- Medical Management: Heart failure or arrhythmias caused by valvular disease may be treated with medications such as ACE inhibitors, beta-blockers, or diuretics.
- Surgical Interventions: Surgery to replace or repair damaged valves may be necessary in cases of significant valvular damage, especially involving the mitral or aortic valves.
5. Long-term Monitoring and Follow-up
- Frequent Check-ups: Patients with a history of rheumatic fever, especially those involving the heart, need regular monitoring by healthcare providers, including ECGs, echocardiograms, and physical examinations.
- Patient Education: Patients and their families should be informed about the importance of completing antibiotic prophylaxis, recognizing early signs of strep throat, and seeking timely treatment to prevent recurrences.
6. Lifestyle Modifications and Preventive Measures
- Avoiding Crowded Areas: Limiting exposure to areas where streptococcal infections are prevalent can help prevent reinfection.
- Early Treatment of Strep Throat: Individuals with a history of rheumatic fever should seek medical attention promptly if they experience any signs of a sore throat to prevent another episode.
- Vaccinations: While there isn’t a specific vaccine for rheumatic fever, staying up-to-date on vaccinations, such as for influenza and pneumonia, can help reduce the overall burden on the immune system.
Prognosis
The degree of cardiac involvement has a major impact on the prognosis of rheumatic fever. Patients with rheumatic heart disease may suffer progressive valve deterioration, which can subsequently cause heart failure, arrhythmias, and other issues. Improving outcomes and preventing long-term complications require early detection, treatment, and prophylaxis.
Conclusion
Rheumatic fever is a serious inflammatory condition that can arise from untreated or insufficiently managed streptococcal throat infections. It primarily affects children and can lead to severe complications, particularly rheumatic heart disease, which is a leading cause of acquired heart disease globally. Prompt diagnosis, effective treatment, and ongoing antibiotic prophylaxis are essential to reduce the risk of permanent cardiac damage and prevent recurring attacks. Public health initiatives, such as improving access to healthcare and promoting the early treatment of streptococcal infections, are crucial in reducing the global burden of this preventable disease.