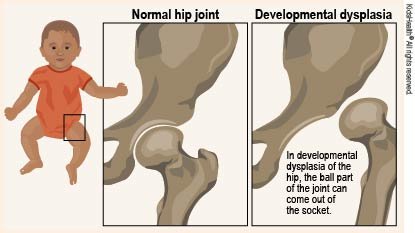
When a baby or young child has developmental dysplasia of the hip (DDH), the hip joint does not grow normally. It includes a range of deformities from a somewhat shallow hip socket to a total dislocation of the joint. Prompt diagnosis and treatment are essential to avoid long-term consequences, such as arthritis and impaired mobility.
Anatomy of the Hip Joint
A ball and socket joint, the hip joint is made up of the acetabulum (socket) and the femoral head (ball). The femoral head slides easily into the acetabulum in a healthy hip, facilitating motion. In DDH, instability results from either an excessively shallow socket or an improperly positioned femoral head.
Causes and Risk Factors
Causes
Though the precise etiology of DDH is unknown, environmental and genetic factors are thought to play a role. These could consist of:
- Genetic Predisposition: The likelihood of DDH is increased in families when the condition runs in the family.
- Mechanical Factors: Limited space in the womb, tight swaddling, and breech presentation during birth can all lead to DDH.
Risk Factors
The following are some of the factors that can raise the risk of DDH:
- Family History: DDH in a close relative.
- Breech Birth: A baby’s birth position when born breech.
- Gender: Affected individuals are more frequently female.
- Firstborn Children: They may be more vulnerable.
- Low Amniotic Fluid: Low levels of amniotic fluid during pregnancy, known as oligohydramnios.
Symptoms
- Leg Length Asymmetry: One leg may seem shorter than the other.
- Limited Hip Abduction: The infant has trouble spreading its legs.
- Asymmetrical Skin Folds: Unequal skin folds in the thigh or buttocks.
- Waddling or Limping Gait: An obvious limp or waddle in older kids.
Diagnosis
Screening
It’s critical to identify DDH early on. Screening usually entails:
- Physical Examination: To screen for hip instability in infants, do the Ortolani and Barlow maneuvers.
- Ultrasound: Used to view the hip joint in babies younger than six months.
- X-rays: Done on older infants and kids to evaluate the growth of the hip joint.
Treatment of Developmental Dysplasia of the Hip
Hip dysplasia (DDH) is a disorder in which the hip joint is malformed and does not fit into the hip socket correctly. Depending on the child’s age and the severity of the ailment, different treatments may be administered.
For Infants (ages 0–6 months)
- Pavlik Harness: A gentle brace that maintains the baby’s hip alignment. Typically, it is worn for several months at a time.
- Hip Abduction Orthosis: A different kind of brace may be employed to hold the hips in the correct position if the Pavlik harness proves to be ineffective.
For Elderly Infants (6–18 months)
- Closed Reduction: This non-surgical technique includes moving the hip joint into position. To hold the hip in place as it heals, casting (also known as a spica cast) is typically applied after.
- Open Reduction: Surgery may be required if closed reduction is unsuccessful or if the child is older. The hip joint is realigned by the surgeon, who may then secure it in place with screws or pins. After that, a spica cast is frequently employed.
For Younger Children and Toddlers (18 months and older)
- Surgical Procedure: In the event that DDH is discovered later, hip joint alignment correction surgery can be necessary. In case of severe joint damage or misalignment, open reduction and perhaps reconstructive surgery may be necessary.
Follow-up Care
- Physical Medicine: To increase mobility and develop the hip-supporting muscles.
- Regular Observation: Regular examinations to make sure the hip is growing normally and to modify treatment as necessary.
Living with Developmental Dysplasia of the Hip (DDH)
1. Adapting to Diagnosis and Treatment
- Recognizing the Situation: Learn about DDH so that you may control expectations and make wise decisions.
- Treatment Plans: Adhere to the recommended treatment plans, which may call for surgery, casts, or braces, in close collaboration with your medical professionals.
2. Daily Life Adjustment
- Managing Mobility: Adjust activities to account for any mobility issues and, if advised, use assistive devices.
- Comfort Measures: If wearing a brace or cast, ensure proper support and comfort. Modify attire and sleeping arrangements as necessary.
3. Physical Therapy and Rehabilitation
- Exercises and Therapy: Follow your doctor’s instructions for physical therapy to strengthen your hip muscles and increase range of motion.
- Engage in Low-Impact Exercises: Support joint health and range of motion without putting undue strain on the hip joint.
4. Support for Emotions and Psychology
- Handling Difficulties: Address any psychological or emotional effects, including frustration or worry, that come with having DDH.
- Support Groups: Consider joining online communities or support groups to connect with people who have gone through similar experiences.
5. Monitoring and Follow-Up
- Frequent Check-Ups: Keep track of your progress and adjust the treatment plan as needed by attending scheduled follow-up appointments.
- Long-Term Monitoring: As the child gets older, watch for any indications of complications or changes in symptoms.
6. Practical Tips for Parents and Caregivers
- Education: Acquire knowledge about DDH and its efficient management to promote the wellbeing of the child.
- Coordination of Treatment: Maintain open communication with educators, therapists, and healthcare professionals to ensure coordinated care and support.
7. Resources and Support
- Educational Resources: Look for books, articles, and online resources to learn more about DDH.
- Expert Assistance: Seek advice from experts including pediatricians, physical therapists, and orthopedic surgeons for comprehensive care.
8. Making Future Plans
- Growth and Development: Plan for future assessments and treatments as the child grows, keeping in mind that ongoing care may be necessary.
- Lifestyle Modifications: Be prepared to adjust your lifestyle as necessary to accommodate any reductions in functionality or mobility.
Conclusion
The hip joint grows abnormally in developmental dysplasia of the hip (DDH), resulting in anything from a shallow socket to a total dislocation. Effective treatment requires an early diagnosis made possible by physical examination, ultrasonography, and X-rays. Younger children may benefit from less invasive techniques like the Pavlik harness, but infants frequently respond better to non-surgical approaches. Physical therapy and ongoing observation are crucial components of follow-up care that guarantee appropriate growth and avert long-term issues. Timely and appropriate treatment can greatly enhance mobility and outcomes.